Antimicrobial Anticoagulant Antibiofilm
Powered by Tetrasodium EDTA


Study Overview
Results from a pragmatic randomized controlled trial to evaluate the effectiveness of 4% t-EDTA in preventing CVAD-associated infections, occlusions, and thrombolytic use in adults treated in an intensive care unit (ICU).

Primary Endpoint
A composite incidence rate of CVAD-associated bloodstream infection (CLABSI), catheter occlusion requiring alteplase use, and/or catheter removal due to occlusion.

Patient Population
ICU patients aged >18 years with CVADs in place and at least 1 lumen not in use.

Sites
6 Canadian hospitals, including 3 community hospitals and 3 academic centers.

Follow Up & Median Length of Stay
Until ICU discharge, death, or the end of the treatment maintenance period. The median length of ICU stay during the study period was 6 days across medical-surgical ICUs (and only 3 days in the cardiac surgery center)
n = 1468
Patients Included
n = 772 Control*
6318 CDs
n = 696 t-EDTA
5654 CDs
*Normal Saline 0.9%; 4% Sodium Citrate HD Catheters;
CD = Catheter Days
Most Commonly Used CVADs
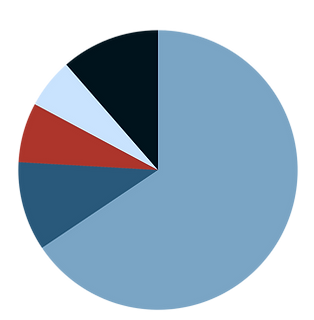
Other
11.4%
Triple Lumen
PICC
5.8%
Trialysis Catheter
6.9%
Hemodialysis
Catheter
10.3%
Triple Lumen
CVC
65.6%
Protocol Compliance
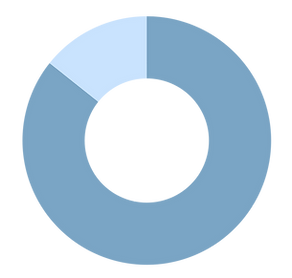
85.7%
1258 patients maintained ≥ 80% adherence to the study proposal
(n = 613, 88% with t-EDTA; n = 645, 84%, 319 control
Results: Primary Outcome Met
Primary Outcome Incidence Rate
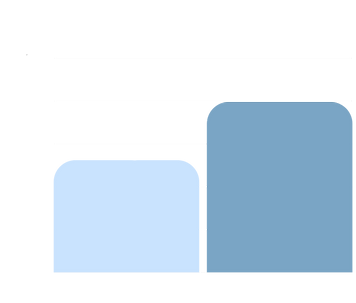
Incidence per 1000 CD
0
5
10
15
20
25
13.1
19.9
34%
fewer events
*p= 0.03
Significantly fewer instances of CLABSI, catheter occlusion requiring alteplase use, and catheter removal due to occlusion were observed with t-EDTA vs control (p= 0.03)*
*In adjusted multivariate analysis of the composite primary outcome
t-EDTA
Control
Secondary Outcomes
0
5
10
15
20
CVAD occlusion requiring administration of alteplase significantly differed in favor of t-EDTA*
CLABSI*
Obstruction Requiring Alteplase
CVAD Removal Due to Occlusion
0.35
0.47
11.67
17.73
1.06
1.74
*The small number of CLABSI limits interpretability of this secondary outcome.
*rate ratio = 0.66
[95% CI: 0.46-0.96]
Incidence per 1000 CD
Safety
No adverse events, serious adverse events, or hypocalcemia related to t-EDTA or control
locking fluid use were reported during the study period.
Liu et al. 2018 https://pubmed.ncbi.nlm.nih.gov/30487154/
Refer to the IFU for Full Safety and Prescribing Information: https://sterilecareinc.com/wp-content/uploads/2025/11/GI_SC001_Catheter-Lock-Solution-3-mL_CA_006-00462_V06_K02.pdf
This information is intended for healthcare professionals and qualified scientific audiences for educational and scientific exchange purposes only.
KiteLock 4% may not be approved, cleared, or authorized in all jurisdictions. Availability, indications, and regulatory status vary by country. Please consult the applicable local product labeling and regulatory status before use. FDA approval pending.